Yusaku Akashi, MD, PhD*1,2,3, Michiko Horie*4, Chisako Yamada*5, Yuto Takeuchi*2,6, Atsuo Ueda*7, Shigeyuki Notake*7, Koji Nakamura*7, Norihiko Terada*6, Yoko Kurihara*6, Hiromichi Suzuki*1,2,6
Akashi Y, Horie M, Yamada C, Takeuchi Y, Ueda A, NOtake S, Nakamura K, Terada N, Kurihara,Y, Suzuki H. A prospective evaluation of Roche’s newly developedSARS-CoV-2 Rapid Antigen Test 2.0 using anterior nasaland nasopharyngeal specimens. Lab Med Int 2025; 4(1): 21-28. doi: 10.51041/lmi.4.1_21
Original
Lab Med Int 2025; 4(1): 21-28
Corresponding author: Division of Infectious Diseases, Department of Medicine, Tsukuba Medical Center Hospital,
1-3-1 Amakubo Tsukuba, Ibaraki 305-8558, Japan.
E-mail: yusaku-akashi”@”umin.ac.jp
Received April 17, 2024; accepted September 6, 2024
*1Department of Infectious Diseases, Faculty of Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8575, Japan
*2Division of Infectious Diseases, Department of Medicine, Tsukuba Medical Center Hospital, 1-3-1 Amakubo Tsukuba, Ibaraki 305-8558, Japan
*3 Akashi Internal Medicine Clinic, 3-1-63 Asahigaoka, Kashiwara, Osaka 582-0026, Japan
*4 Roche Diagnostics K.K, Medical Scientific Affairs Group, Shinagawa Season Terrace 1-2-70, Konan, Minato-ku, Tokyo, 108-0075, Japan
*5 Roche Diagnostics K.K, Customer Care Group, Shinagawa Season Terrace 1-2-70, Konan, Minato-ku, Tokyo, 108-0075, Japan
*6 Department of Infectious Diseases, University of Tsukuba Hospital, 2-1-1 Amakubo, Tsukuba, Ibaraki 305-8576, Japan
*7 Department of Clinical Laboratory, Tsukuba Medical Center Hospital, 1-3-1 Amakubo, Tsukuba, Ibaraki 305-8558, Japan
ABSTRACT
Rapid qualitative antigen tests are essential for the management of COVID-19, but their sensitivity and specificitazy vary. This study prospectively evaluated the diagnostic performance of a newly developed product, the SARS-CoV-2 Rapid antigen test 2.0 (Roche Diagnostics GmbH, Mannheim, Germany) in anterior nasal and nasopharyngeal samples, comparing results with reverse transcription polymerase chain reaction(RT-PCR)in nasopharyngeal samples. The symptomatic participants or asymptomatic participants with a history of close contact with COVID-19 patients were consecutively enrolled. The study also evaluated the sensitivities across different viral loads in pooled samples with known viral RNA levels and compared them with those of a previous product.
Among 287 participants, 283 were symptomatic and 187 tested positive for SARS-CoV-2; 179 nasopharyngeal samples had viral loads ≥ 1,000 copies/test. The antigen test had a sensitivity of 92.5% (95% confidence interval [CI]: 87.8%-95.8%) and specificity of 100% (95% CI: 96.4%-100%) in anterior nasal samples. When stratified by viral loads in the corresponding nasopharyngeal samples(≥105, ≥104 to <105 , ≥103 to <104, ≥102 to <103, and <102 viral copies/test), the sensitivities were 95.9%, 91.3%, 70.0%, 100%, and 40%, respectively. For nasopharyngeal samples, the sensitivity and specificity of the antigen test were 97.3%(95% CI: 93.9%-99.1%)and 99.0%(95% CI: 94.6%-100%), respectively. In the evaluation of pooled samples, the SARS-CoV-2 Rapid antigen test 2.0 demonstrated a lower limit of detection for SARS-CoV-2 compared to the previous product.
The SARS-CoV-2 Rapid antigen test 2.0 exhibited sufficient diagnostic performance, with improved detection performance over the previous products.
〔Lab Med Int 2025; 4(1): 21-28〕
Key Words
lateral flow qualitative antigen testing, COVID-19, nasal and nasopharyngeal samples, Point-of-Care testing, SARS-CoV-2 Rapid antigen test 2.0
I. INTRODUCTION
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has been prevailing and causing coronavirus disease (COVID-19) worldwide 1). Despite advancements in treatments and vaccination efforts, COVID-19 continues to pose a significant health threat to vulnerable populations 1), underscoring the critical need for prompt and accurate diagnosis for effective infection control. While molecular examinations are the gold standard for COVID-19 diagnosis because of their high reliability 2), rapid antigen tests have been widely used due to their convenience, immediate results, and wide availability 3).
Prior to the emergence of the Omicron variant and other subsequent variants, the SARS-CoV-2 Rapid antigen test (Roche Diagnostics GmbH, Mannheim, Germany) showed sufficient sensitivity and specificity in nasopharyngeal samples 4). However, our previous study revealed a significant decrease in the test’s sensitivity for samples containing low viral load, e.g., anterior nasal samples 4). As such, re-evaluating and improving the diagnostic performance of this product seem warranted.
The SARS-CoV-2 Rapid antigen test 2.0 (Roche Diagnostics GmbH, Mannheim, Germany) is an improved version of the SARS-CoV-2 Rapid antigen test using new reagents but its utility with clinical samples has not yet been evaluated. In this study, we conducted a prospective evaluation of the diagnostic performance of the SARS-CoV-2 Rapid antigen test 2.0 using both anterior nasal and nasopharyngeal samples. Additionally, we assessed its sensitivity across a range of viral loads by analyzing pooled samples with known quantities of viral RNA.
II. MATERIALS AND METHODS
The evaluations were performed at a drive-through PCR center in Tsukuba Medical Center Hospital (TMCH; Tsukuba, Japan) between August 16 and August 29, 2022. All of the participants were referred for SARS-CoV-2 RT-PCR from 42 clinics and a local public health center as previously described 5)6). The study included participants having symptoms compatible with COVID-19 or a history of close contact with COVID-19 patients if they were asymptomatic. The results of the SARS-CoV-2 Rapid antigen test 2.0 were compared with those of RT-PCR with nasopharyngeal samples. One anterior nasal sample and two nasopharyngeal samples were simultaneously collected from participants after obtaining their verbal informed consent. The informed consent process was performed verbally to prevent infection transmission and was documented in the corresponding electronic medical record. The ethics board of the University of Tsukuba approved the protocol (approval number: R03-041).
Sample collection and antigen testing with SARS-CoV-2 Rapid antigen test 2.0
Anterior nasal samples were first obtained from both nostrils, as previously described 4), and two nasopharyngeal samples were then collected for antigen testing and RT-PCR following the recommended procedure 7). The swab included in the antigen test kits was used for antigen testing, and a FLOQSwab (Copan ItaliaSpA, Brescia, Italy) was used for RT-PCR. All sample collections were performed by trained medical staff. Antigen testing was performed immediately after sample collection.
Procedures for RT-PCR examinations
For RT-PCR, swabs collected from the nasopharynx were suspended in 3 mL of Universal Transport Medium (UTM; Copan Italia SpA) and preserved at −80℃ after in-house RT-PCR at the TMCH microbiology department. The in-house RT-PCR was performed primarily for clinical purposes and its procedures for in-house RT-PCR have been described previously 8)9). Briefly, purification and RNA extraction were performed using a magLEAD 6gC (Precision System Science Co., Ltd., Chiba, Japan) from 200 µL aliquots of UTM. The GENECUBE® (TOYOBO Co., Ltd., Osaka, Japan) and GENECUBE® HQ SARS-CoV-2 assays, which target the N region, were used for detecting SARS-CoV-2. The UTM was then transported to LSI Medience Corporation (Tokyo, Japan) for reference RT-PCR testing.
As a reference, real-time RT-PCR at LSI Medience Corporation was performed using the national standard method developed by the National Institute of Infectious Diseases (NIID), Japan 5)10)–13). The purification and RNA extraction were performed on 200-μL aliquots of UTM samples using the Maxwell® RSC Viral Total Nucleic Acid Purification Kit and Maxwell® RSC 48 Instrument (Promega Corporation, Madison, WI, USA). The NIID test targets the N2 region, and the RT-PCR equipment included the cobas® z480 (Roche Diagnostics International Ltd., Rotkreuz, Switzerland), the QuantiTect® Probe RT-PCR Kit (QIAGEN, Hilden, Germany), and a SARS-CoV-2 standard (Exact Diagnostics LLC, Fort Worth, TX, USA). Viral loads were quantified using the NIID N2 method with calibration curves generated from EDX SARS-CoV-2 Standard (Bio-Rad Laboratories, Inc., Hercules, CA, USA) at concentrations of 100, 125, 250, 500, and 1000 copies/reaction. The average viral load of the duplicate assays per sample was used for analysis.
Samples with discrepancies between in-house RT-PCR and NIID N2 RT-PCR underwent further testing using the cobas® Liat® system and cobas® Liat SARS-CoV-2 & Influenza A/B (Liat; Roche Molecular Systems, Inc., Pleasanton, CA, USA)14)–16). The Liat assays were exclusively used for resoloving the discordance, with their results considered definitive for determining the SARS-CoV-2 status of the sample.
Evaluation of limit of detection of the SARS-CoV-2 Rapid antigen test 2.0 and the SARS-CoV-2 Rapid antigen test
To evaluate the limit of detection (LOD) for SARS-CoV-2 using the SARS-CoV-2 Rapid antigen test 2.0, we prepared samples of 7 concentrations for the evaluation by serially diluting 4 pooled positive samples with 5 negative matrix samples (UTM; four pooled nasopharyngeal samples). The 4 pooled positive samples were prepared from preserved UTM media of participants previously diagnosed with COVID-19.
For each concentration, 20 samples were prepared, resulting in a total of 140 samples for the study. The LOD evaluation was performed concurrently with the SARS-CoV-2 Rapid antigen test 2.0 and the SARS-CoV-2 Rapid antigen test.
For antigen testing with both kits, 350 μL of each of the 140 specimens were added with an equal volume of the extraction buffer provided in the antigen kit. The antigen tests were performed following the manufacturer’s instructions, and the interpretation of the antigen test results was carried out by two independent medical technicians in a blinded manner. To ensure blinding, all samples were randomly numbered by other researchers before being provided to the technicians. The limit of detection (LOD) was defined as the viral concentration at which both examiners achieved a detection sensitivity of >95%.
Statistical analyses
The sensitivity and specificity of the antigen tests were calculated with 95% confidence intervals (CIs). The sensitivity was stratified according to the viral loads assessed by the N2 set of the NIID method. If a sample had tested negative on the NIID N2 RT-PCR but positive on the in-house RT-PCR and Liat assay, it would have been considered to have a minimal viral load of < 100 copies/test.
All statistical analyses were conducted using the R 4.1.2 software program (R Foundation, Vienna, Austria) with the “readxl,” “tidyverse,” and “epiR” packages.
III. RESULTS
In this study, 287 participants were assessed, and 283 (98.6%) were found to be symptomatic. The median interval from symptom onset to sample collection was 1.0 days (IQR: 1.0-2.0 days). The NIID N2 assays were positive in 185 samples and negative in 102 samples, among which the results of 5 samples were different from those of in-house RT-PCR tests. Of the 5 samples, the Liat assays were positive in 3 and negative in 2 (Supplementary Table 1). As a result, we considered SARS-CoV-2 to be positive in 187 (65.2%) and negative in 100 samples (34.8%).
Diagnostic performance of SARS-CoV-2 Rapid antigen test 2.0 in anterior nasal samples
Table 1 shows the diagnostic performance of SARS-CoV-2 Rapid antigen test 2.0 in anterior nasal samples. The overall sensitivity and specificity were 92.5% (95% CI: 87.8%–95.8%) and 100% (95% CI: 96.4%–100%), respectively. When stratified by viral loads of copies/test (with ≥105, ≥104 to <105 , ≥103 to <104, ≥102 to <103, and <102) in the corresponding nasopharyngeal samples, the sensitivities were 95.9% (95% CI: 91.3%–98.5%), 91.3% (95% CI: 72.0%–98.9%), 70.0% (95% CI: 34.8%–93.3%), 100% (29.2%–100%), and 40.0% (95% CI: 0%–84.2%), respectively (Table 2).
Diagnostic performance of SARS-CoV-2 Rapid antigen test 2.0 in nasopharyngeal samples
The SARS-CoV-2 Rapid antigen test 2.0 demonstrated an overall sensitivity of 97.3% (95% CI: 93.9–99.1%) and specificity of 99.0% (95% CI: 94.6–100%) when using nasopharyngeal samples (Table 3). As shown in Table 4, the sensitivities of the SARS-CoV-2 Rapid antigen test 2.0 for nasopharyngeal samples with viral loads of ≥105, ≥104 to <105, ≥103 to <104, ≥102 to <103, and <102 copies/test were 99.3% (95% CI: 96.2–100%), 100% (95% CI: 85.2–100%), 90.0% (95% CI: 55.5–99.7%), 100% (95% CI: 29.2–100%), and 40% (95% CI: 5.3–85.3%), respectively.
Table 5 summarizes the variation in sensitivity of the SARS-CoV-2 Rapid antigen test 2.0 according to days since symptom onset. While sensitivity in anterior nasal samples increased from 86.7% on day 0 to 100% from day 3 onwards, nasopharyngeal samples consistently demonstrated a sensitivity exceeding 90% throughout the observation period.
Evaluation and comparison of the limit of detection of the SARS-CoV-2 Rapid antigen test 2.0 and the SARS-CoV-2 Rapid antigen test
For the SARS-CoV-2 Rapid antigen test 2.0, both investigators reported 100% detection rates at concentrations of 6,250 copies/test and higher on the corresponding UTM samples (Table 6). In contrast, for the SARS-CoV-2 Rapid antigen test, both investigators demonstrated 100% detection rates up to a concentration of 12,500 copies/test. The complete dataset was provided as Supplementary Table 2.
IV. DISCUSSION
Among anterior nasal and nasopharyngeal samples, the SARS-CoV-2 Rapid antigen test 2.0 demonstrated high sensitivities of 92.5% and 97.3%, retaining specificities of 100% and 99.0%, respectively. In addition, the analysis of pooled positive samples in this study also suggested a lower LOD of SARS-CoV-2 Rapid antigen test 2.0 compared to its previous product.
The anterior nostrils generally have a lower viral load than the nasopharynx 17). In fact, according to our previous study, the SARS-CoV-2 Rapid antigen test showed a modest sensitivity of 72.7% in anterior nasal samples 4). However, in the current study, the diagnostic performance of the SARS-CoV-2 Rapid antigen test 2.0 was high and comparable for both sample types. A notable difference in sensitivity existed only in samples with viral loads of 103–104 copies/test, with sensitivities of 70.0% and 90.0% for anterior nasal and nasopharyngeal samples, respectively (Table 2 and Table 4). This finding suggests that the sensitivity of the current product has improved compared to the SARS-CoV-2 Rapid antigen test. In addition, our pooled sample analysis, which showed a better LOD for the SARS-CoV-2 Rapid antigen test 2.0 than for the original SARS-CoV-2 Rapid antigen test, provides further evidence of its improved sensitivity.
The high sensitivity of the SARS-CoV-2 Rapid antigen test 2.0 in anterior nasal samples can increase the utility of antigen tests. Anterior nasal sample collections may prevent the induction of cough or sneezing during sample collection, thus reducing virus transmission from patients 18). In addition, anterior nasal sample collection is less burdensome and more suitable for self-testing than nasopharyngeal collection 19). Despite showing a slight decrease in sensitivity on the first and following days of symptom onset (Table 5), the SARS-CoV-2 Rapid antigen test 2.0 maintains good performance with anterior nasal samples. The availability of several antigen tests as over-the-counter products has contributed to the increasing popularity and widespread use of self-testing. The good sensitivity of the SARS-CoV-2 Rapid antigen test 2.0 in anterior nasal samples may further promote the adoption of this sampling method, making testing more accessible and convenient for the general population.
Differences in genome variants of SARS-CoV-2 are another factor that can influence the diagnostic performance of antigen tests. The study period during which this evaluation was performed was the “7th wave” of COVID-19 in Japan, where the Omicron BA4/5 variant was dominant. Compared to the Omicron BA.1 variant, Roche’s previous product, SARS-CoV-2 Rapid antigen test, showed a reduced sensitivity for the BA.2, BA.5 variant 20). Despite this, the SARS-CoV-2 Rapid antigen test 2.0 demonstrated adequate analytical performance with both anterior nasal and nasopharyngeal samples, although the current study did not analyze the genome variant. It is important to note that the diagnostic performance of antigen tests can change with the emergence of other variants and should be continuously evaluated.
Several limitations associated with the present study warrant mention. First, the study population consisted primarily of symptomatic participants, with the majority of corresponding nasopharyngeal UTM samples containing viral loads greater than 104 copies/test. Nevertheless, two previous studies have reported similar sensitivities for this antigen test, with 92.9% for nasal samples 21) and 92.1-92.9% for nasopharyngeal samples 21)22), which are consistent with our findings. Second, the use of frozen samples may have influenced the reference test results. Third, the study did not evaluate the potential impact of vaccination status or medication use on the diagnostic performance of the test. Finally, this study’s LOD evaluation used samples stored in UTM, while direct inoculation of sampled swabs into the antigen extraction medium is the standard practice in clinical settings. This may have influenced the tests’ performance 23)–25) and should be considered when interpreting the results of this study.
In conclusion, this first clinical evaluation of the SARS-CoV-2 Rapid antigen test 2.0 showed a sufficient diagnostic performance with both anterior nasal and nasopharyngeal samples. In addition, the product showed an improvement in its LOD for SARS-CoV-2. These results support the clinical utility of the new product for detecting SARS-CoV-2 and highlight the importance of continuous evaluation and improvement of rapid antigen tests.
Table 1 Diagnostic performance of the SARS-CoV-2 Rapid antigen test 2.0 with anterior nasal samples
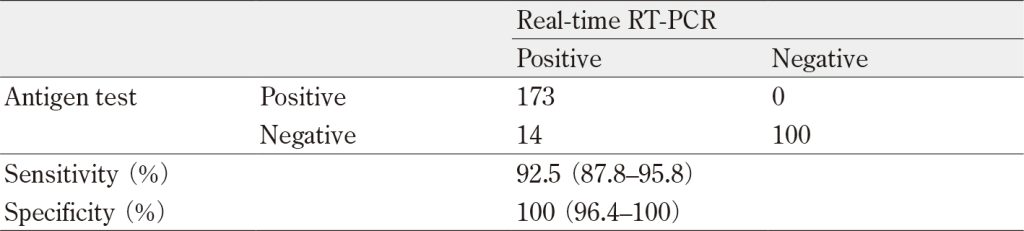
RT-PCR, reverse transcription-polymerase chain reaction
Data in parentheses indicate 95% confidence intervals.
Table 2 Sensitivity of the SARS-CoV-2 Rapid antigen test 2.0 with anterior nasal samples stratified by viral loads of RT-PCR with nasopharyngeal samples
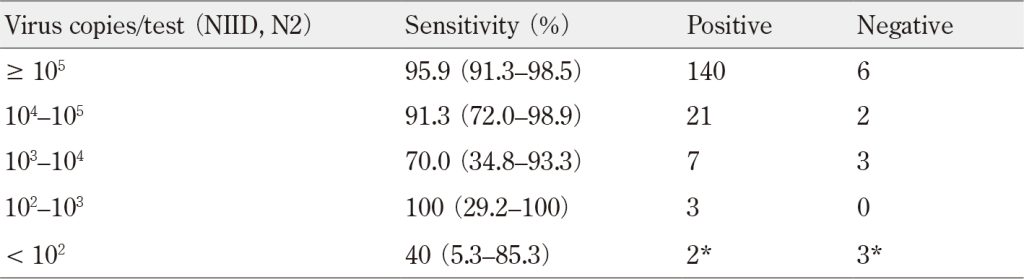
NIID, National Institute of Infectious Diseases(NIID), Japan; RT-PCR, reverse transcription-polymerase chain reaction
*The viral loads of three SARS-CoV-2 positive samples, which tested negative on the NIID N2 assay but positive on both the in-house PCR and Liat assay, were determined to be below 100 copies/test.
Data in parentheses indicate 95% confidence intervals.
The viral loads for RT-PCR were determined using the NIID( N2 gene), Japan method
Table 3 Diagnostic performance of the SARS-CoV-2 Rapid antigen test 2.0 with nasopharyngeal samples
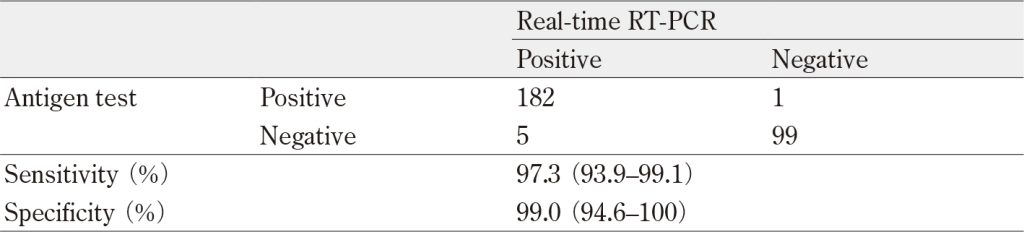
RT-PCR, reverse transcription-polymerase chain reaction
Data in parentheses indicate 95% confidence intervals.
Table 4 Sensitivity of the SARS-CoV-2 Rapid antigen test 2.0 with nasopharyngeal samples stratified by viral loads of RT-PCR with nasopharyngeal samples
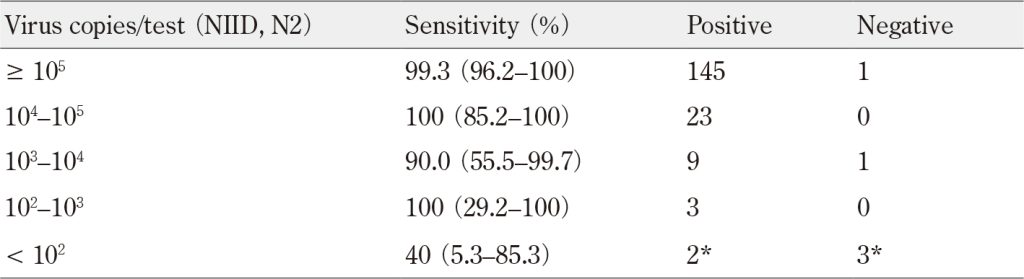
NIID, National Institute of Infectious Diseases (NIID), Japan; RT-PCR, reverse transcription-polymerase chain reaction
* The viral loads of three SARS-CoV-2 positive samples, which tested negative on the NIID N2 assay but positive on both the in-house PCR and Liat assay, were determined to be below 100 copies/test.
Data in parentheses indicate 95% confidence intervals.
The viral loads for RT-PCR were determined using the NIID( N2 gene), Japan method
Table 5 Sensitivity of the SARS-CoV-2 Rapid antigen test 2.0 stratified by the number of days since symptom onset
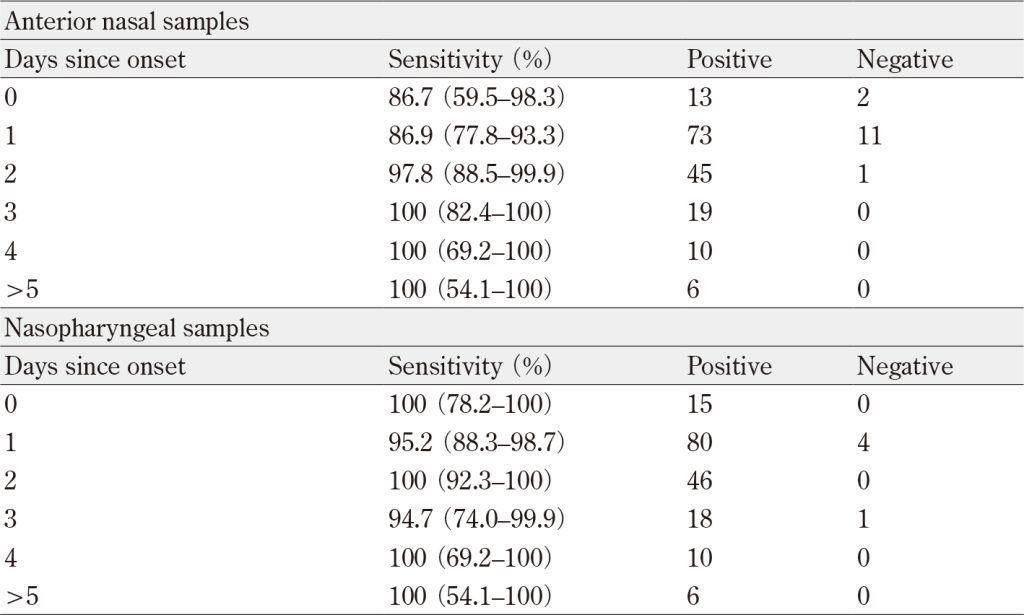
Of the 283 symptomatic participants included in the data, onset date was unavailable for 11.
Data in parentheses indicate 95% confidence intervals.
Table 6 Detection rates of SARS-CoV-2 Rapid antigen test 2.0 and SARS-CoV-2 Rapid antigen test at different
viral concentrations using pooled positive samples
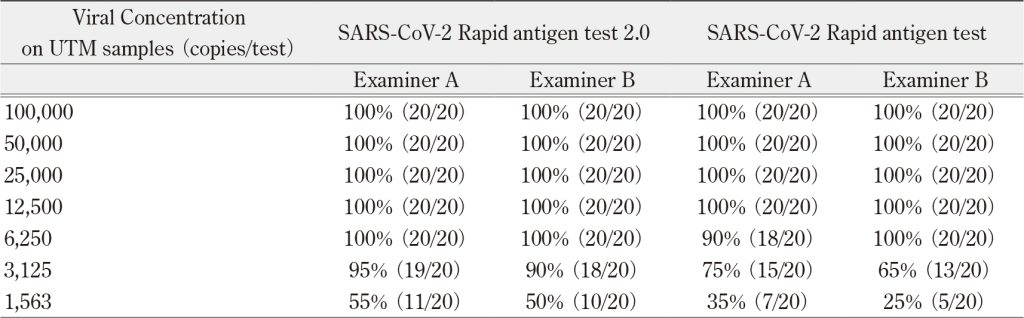
UTM, Universal Transport Medium
The values in parentheses represent the number of positive samples detected out of the total number of samples
tested at each concentration.
ACKNOWLEDGEMENTS
COBAS and LIAT are trademarks of Roche. SARS-CoV-2 Rapid antigen test 2.0 is manufactured by SD Biosensor and distributed by Roche Diagnostics.
AUTHORSHIP CONTRIBUTIONS
All authors meet criteria for authorship set by the International Committee of Medical Journal Editors. Yusaku Akashi was the principal investigator, wrote the first draft of the manuscript, and performed the statistical analyses. Michiko Horie and Hiromichi Suzuki designed the study. Chisako Yamada performed the molecular testing using the cobas® Liat® system and cobas® Liat SARS-CoV-2 & Influenza A/B. Atsuo Ueda, Shigeyuki Notake and Koji Nakamura collected the samples and performed the diagnostic tests. Hiromichi Suzuki supervised the project. All authors contributed to writing the final draft of the manuscript.
DISCLOSURE OF CONFLICT OF INTERESTS
Roche Diagnostics, Co., Ltd financially supported this study and provided remuneration to Michiko Horie and Chisako Yamada. Hiromichi Suzuki received lecture fees from Roche Diagnostics K.K.
References
- World Health Organization. Weekly epidemiological update on COVID-19-5 October 2022. [cited 2022 Oct 10]. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—5-october-2022
- Centers for Disease Control and Prevention. Nucleic Acid Amplification Tests (NAATs). [cited 2022 Oct 10] Available from: https://www.cdc.gov/coronavirus/2019-ncov/lab/naats.html
- Centers for Disease Control and Prevention. Guidance for Antigen Testing for SARS-CoV-2 for Healthcare Providers Testing Individuals in the Community. [cited 2022 Oct 11]. Available from: https://stacks.cdc.gov/view/cdc/115045
- Akashi Y, Horie M, Takeuchi Y, et al. A prospective clinical evaluation of the diagnostic accuracy of the SARS-CoV-2 rapid antigen test using anterior nasal samples. J Infect Chemother 2022; 28(6): 780-5. doi: 10.1016/j.jiac.2022.02.016.PubMed
- Takeuchi Y, Akashi Y, Kiyasu Y, et al. A prospective evaluation of diagnostic performance of a combo rapid antigen test QuickNavi-Flu+COVID19 Ag. J Infect Chemother 2022; 28(6): 840-3. doi: 10.1016/j.jiac.2022.02.027.PubMed
- Suzuki H, Akashi Y, Kato D, et al. Analytical performance of the rapid qualitative antigen kit for the detection of SARS-CoV-2 during widespread circulation of the Omicron variant. J Infect Chemother 2023; 29(3): 257-62. doi: 10.1016/j.jiac.2022.11.006.PubMed
- Marty FM, Chen K, Verrill KA. How to Obtain a Nasopharyngeal Swab Specimen. N Engl J Med 2020; 382(22): e76. doi: 10.1056/NEJMvcm2010260.PubMed
- Naito A, Kiyasu Y, Akashi Y, et al. The evaluation of the utility of the GENECUBE HQ SARS-CoV-2 for anterior nasal samples and saliva samples with a new rapid examination protocol. PLoS One 2021; 16(12): e0262159. doi: 10.1371/journal.pone.0262159.PubMed
- Kiyasu Y, Akashi Y, Sugiyama A, et al. A Prospective Evaluation of the Analytical Performance of GENECUBE® HQ SARS-CoV-2 and GENECUBE® FLU A/B. Mol Diagn Ther 2021; 25(4): 495-504. doi: 10.1007/s40291-021-00535-5.PubMed
- Shirato K, Nao N, Katano H, et al. Development of Genetic Diagnostic Methods for Detection for Novel Coronavirus 2019(nCoV-2019)in Japan. Jpn J Infect Dis. 2020; 73(4): 304-7. doi: 10.7883/yoken.JJID.2020.061.PubMed
- Akashi Y, Kiyasu Y, Takeuchi Y, et al. Evaluation and clinical implications of the time to a positive results of antigen testing for SARS-CoV-2. J Infect Chemother. 2022; 28(2): 248-51. doi: 10.1016/j.jiac.2021.10.026.PubMed
- Ishikane M, Unoki-Kubota H, Moriya A, et al. Evaluation of the QIAstat-Dx Respiratory SARS-CoV-2 panel, a rapid multiplex PCR method for the diagnosis of COVID-19. J Infect Chemother 2022; 28(6): 729-34. doi: 10.1016/j.jiac.2022.02.004.PubMed
- Tsujimoto Y, Terada J, Kimura M, et al. Diagnostic accuracy of nasopharyngeal swab, nasal swab and saliva swab samples for the detection of SARS-CoV-2 using RT-PCR. Infect Dis(Lond). 2021; 53(8): 581-9. doi: 10.1080/23744235.2021.1903550.PubMed
- Akashi Y, Horie M, Kiyotaki J, et al. Clinical Performance of the cobas Liat SARS-CoV-2 & Influenza A/B Assay in Nasal Samples. Mol Diagn Ther 2022; 26(3): 323-31. doi: 10.1007/s40291-022-00580-8.PubMed
- Blackall D, Moreno R, Jin J, et al. Performance Characteristics of the Roche Diagnostics cobas Liat PCR System as a COVID-19 Screening Tool for Hospital Admissions in a Regional Health Care Delivery System. J Clin Microbiol. 2021; 59(10): e0127821. doi: 10.1128/JCM.01278-21.PubMed
- Mahmoud SA, Ganesan S, Ibrahim E, et al. Evaluation of six different rapid methods for nucleic acid detection of SARS-COV-2 virus. J Med Virol 2021; 93(9): 5538-43. doi: 10.1002/jmv.27090.PubMed
- Zhou Y, O’Leary TJ. Relative sensitivity of anterior nares and nasopharyngeal swabs for initial detection of SARS-CoV-2 in ambulatory patients: Rapid review and meta-analysis. PLoS One 2021; 16(7): e0254559. doi: 10.1371/journal.pone.0254559.PubMed
- Takeuchi Y, Akashi Y, Kato D, et al. Diagnostic performance and characteristics of anterior nasal collection for the SARS-CoV-2 antigen test: a prospective study. Sci Rep 2021; 11(1): 10519. doi: 10.1038/s41598-021-90026-8.PubMed
- Waggoner JJ, Vos MB, Tyburski EA, et al. Concordance of SARS-CoV-2 Results in Self-collected Nasal Swabs vs Swabs Collected by Health Care Workers in Children and Adolescents. JAMA 2022; 328(10): 935-40. doi: 10.1001/jama.2022.14877.PubMed
- Leuzinger K, Roloff T, Egli A, et al. Impact of SARS-CoV-2 Omicron on Rapid Antigen Testing Developed for Early-Pandemic SARS-CoV-2 Variants. Microbiol Spectr 2022; 10(4): e0200622. doi: 10.1128/spectrum.02006-22.PubMed
- Widyasari K, Kim S. Efficacy of novel SARS-CoV-2 rapid antigen tests in the era of omicron outbreak. PLoS One. 2023; 18(8): e0289990. doi: 10.1371/journal.pone.0289990.PubMed
- Flinck H, Aittoniemi J. Evaluation of the new 2.0 version of the Roche SARS-CoV-2 Rapid Antigen Test. J Virol Methods 2023; 319: 114758. doi: 10.1016/j.jviromet.2023.114758.PubMed
- Takeuchi Y, Akashi Y, Kato D, et al. The evaluation of a newly developed antigen test(QuickNaviTM-COVID19 Ag)for SARS-CoV-2: A prospective observational study in Japan. J Infect Chemother 2021; 27(6): 890-4. doi: 10.1016/j.jiac.2021.02.029.PubMed
- Kiyasu Y, Takeuchi Y, Akashi Y, et al. Prospective analytical performance evaluation of the QuickNaviTM-COVID19 Ag for asymptomatic individuals. J Infect Chemother 2021; 27(10): 1489-92. doi: 10.1016/j.jiac.2021.07.005PubMed
- Yamayoshi S, Sakai-Tagawa Y, Koga M, et al. Comparison of Rapid Antigen Tests for COVID-19. Viruses 2020; 12(12): 1420. doi: 10.3390/v12121420.PubMed